

Abstract
Background: Adult T-Cell Lymphoma/Leukemia (ATLL) is a rare and aggressive HTLV-1 related peripheral T-cell lymphoma that occurs predominantly in Japan and the Caribbean basin. Acute (A) and lymphomatous (L) subtypes are the most aggressive forms with a median overall survival (OS) of 6-12 months despite chemotherapy. Typical immunophenotype (IP) of ATLL is CD4+/CD8- with strong co-expression of CD25. Atypical IP has been reported in ~10-20% of cases, and has been linked to a more aggressive disease in rare Japanese case reports. However, little literature exists on the Caribbean population. Kings County Hospital (KCH) and University Hospital of Brooklyn (UHB) serve a big Caribbean community in Brooklyn, New York. Our primary objective is to describe the clinicopathologic characteristics and treatment outcomes of our Caribbean patients. We also aim to evaluate the effect of IP on prognosis.
Methods: We conducted a retrospective analysis of all patients diagnosed with HLTV1+ ATLL at KCH and UHB between 2005 and 2017. Diagnosis of ATLL was established based on clinical history, pathological findings and HTLV1 serum positivity. We included patients with A and L subtypes only. IP was based on flow cytometry from peripheral blood and/or immunostaining from lymph node biopsy. For the univariate analysis, outcomes were calculated using the log-rank test, and survival curves were estimated by Kaplan-Meier method.
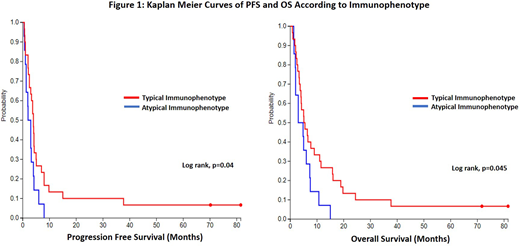
Results: We identified 63 patients with A and L subtypes. The median age was 54 with female predominance (65%). A and L subtypes were noted in 55% and 45% of patients respectively, and 95% had Ann Arbor stage III/IV. Two patients transformed to A subtype from chronic disease, and one patient transformed to L subtype from smoldering disease. Organ involvement at presentation was as follows: lymphadenopathy (80%), bone marrow (63%), hepatomegaly (25%), skin lesions (24%), bone lesions (23%), splenomegaly (21%), pleural effusions (14%), lung (11%), and CNS (8%). Hypercalcemia was noted in 47%, and only 4 patients had normal LDH. Out of 26 patients with a reported karyotype, 8 patients had abnormal cytogenetics (31%). Most patients received upfront EPOCH (78%) or CHOP chemotherapy (14%). The objective response rate (ORR) was 47% (complete response [CR] 16%, partial response [PR] 31%) and stable disease (SD) was achieved in 14%. None of the patients received antiviral therapy or consolidative stem cell transplant. The median duration of response was 2.1 months. The median OS was 5.8 months and median progression-free survival (PFS) was 4 months. Strikingly, 4 patients survived beyond 3 years including two who remain alive at 5+ years without further therapy. Of patients with relapsed/refractory (R/R) disease (85%), 35 patients (66%) received 2nd line treatment (mostly ICE chemotherapy: 27%). ORR was 21% (1 CR and 6 PR) and another patient had SD. For R/R patients, the median OS was 2.2 months and median PFS was 2 months. Univariate analysis showed that the following factors were associated with shorter OS and PFS: LDH > twice the upper limit of normal (p=0.002 and <0.001, respectively), bone marrow involvement (p<0.001), hypercalcemia >13 mg/dl (p<0.001), and absence of response to first line chemotherapy (p<0.001). Abnormal cytogenetics correlated with shorter PFS (p=0.04) but not OS (p=0.13). 14 patients had atypical IP (32%) with the following distribution: CD4- (3 patients), CD4+/CD8+ (3 patients), CD4-/CD8- (2 patients), CD25 dim (5 patients) and CD25- (1 patient). Among those who received chemotherapy, atypical IP was associated with shorter OS (p=0.04) and PFS (p=0.04) (Figure 1). Normal LDH correlated with OS beyond 1 year.
Conclusion: Our large cohort of Caribbean patients with acute and lymphomatous subtypes of ATLL suggests a chemo-refractory and more aggressive disease compared with Japanese population, highlighting the need for novel therapies. In our patient population, incidence of atypical immunophenotype was higher than previously reported and was associated with worse PFS and OS.
Disclosures: No relevant conflicts of interests to declare.
No relevant conflicts of interest to declare.

